SHM Publishes Policy Statement Addressing the Opioid Epidemic
May 10, 2018
SHM's Policy Efforts
SHM supports legislation that affects hospital medicine and general healthcare, advocating for hospitalists and the patients they serve.
Policy Position Statement: Addressing the Opioid Epidemic
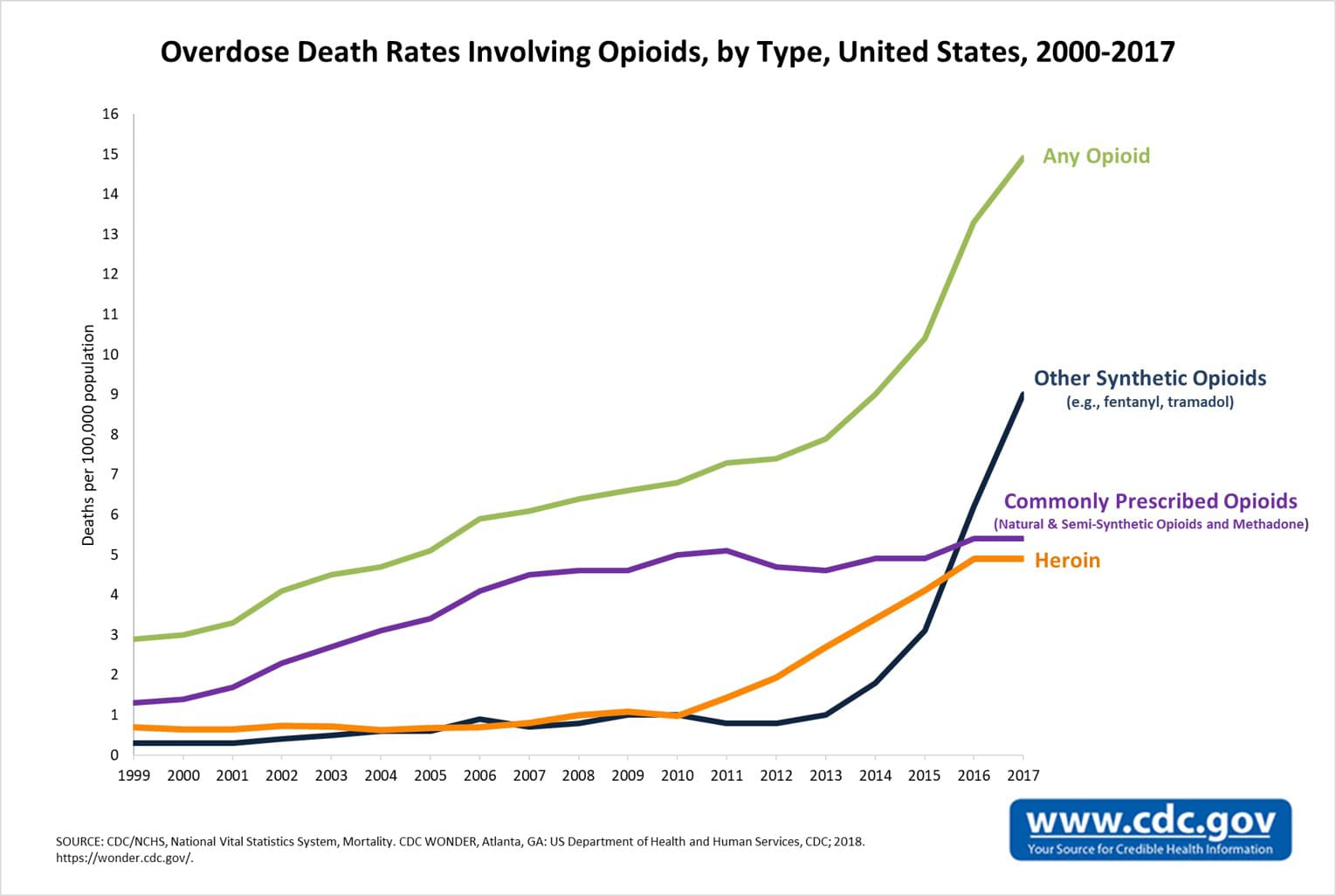
The Society of Hospital Medicine (SHM), representing the nation’s hospitalists, urges Congress to take action to address the opioid crisis facing the United States. Overdose on opioids is a daunting epidemic, with an estimated 115 persons dying each day.1 This is a multifaceted problem, impacting people and families in every community, and it requires intervention on multiple fronts.
Hospitalists are front-line healthcare providers in America’s hospitals, caring for millions of hospitalized patients each year, including more than half of all hospitalized Medicare beneficiaries. As leaders of an interdisciplinary care team, hospitalists manage the inpatient medical needs of patients, which includes addressing acute and chronic pain during a hospital stay and at discharge.
We believe all providers, including hospitalists, have an important role in addressing the opioid epidemic. SHM recently convened a workgroup of hospitalist experts to craft a consensus guidance statement on opioid prescribing during acute hospitalizations. This statement, published in April 20182, includes recommendations on when to prescribe opioids in the hospital and how to improve the safety of opioid prescribing during hospitalization and discharge. These recommendations, if implemented into practice, are a key part of a comprehensive strategy for safe opioid prescribing.
We also believe there is significant opportunity for federal policy changes that would help address this crisis. We detail our policy recommendations below:
1. Expand access to buprenorphine
Buprenorphine is a partial opioid agonist that can be used to treat opioid addiction. It is an important tool, particularly when combined with counseling or behavioral therapy, in combatting opioid use disorder (OUD). To prescribe buprenorphine, physicians must submit to the requirements of the Drug Addiction Treatment Act of 2000, including applying for a waiver. We encourage Congress to revisit the waiver requirements and deregulate prescribing authority, or further streamline the process by which providers receive permission to prescribe buprenorphine. This should be coupled with increased education and training for providers in detecting and treating OUD.
2. Reduce adverse incentives for opioid prescribing
Congress should consider the adverse incentives that create the potential for opioid overprescribing. Quality measures and other federal assessments of both providers and facilities must be harmonized to encourage the expansion of non-opioid treatment of pain. In 2016-2017, the Centers for Medicare & Medicaid Services enacted changes to the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) questions after hearing concerns hospitalists and other healthcare stakeholders raised about the potential for pain assessment questions to inadvertently encourage opioid prescribing. The HCAHPS pain management questions may require further study and adjustment, as we gain a greater understanding of how measures can drive prescribing behavior. Other measures throughout federal programs should also be reviewed to ensure they do not unintentionally encourage unnecessary prescribing.
3. Improve Prescription Drug Monitoring Programs (PDMPs) by driving forward interoperability and integration into electronic medical records (EMRs)
Prescription Drug Monitoring Programs (PDMPs) are databases managed by states or other entities to collect information on a variety of controlled substances. As part of best practices for prescribing, clinicians should review their state PDMP as part of their decision-making process for opioid therapy. However, several barriers exist that impede the effectiveness and usability of PDMPs and make it difficult for providers to use these tools in their practice.
Interoperability: there is no consistent data sharing across state lines or on a national level, although some states do participate in a data-sharing hub. Without data from surrounding localities, PDMPs do not provide clinicians with the full prescribing picture for their patients. The ability to see nationwide data on opioid prescribing would enable clinicians to better detect patterns of abuse and encourage their patients to seek treatment. Legislation is needed to establish a national PDMP or to support efforts for broad information exchange to ensure this vital information is fully disseminated.
Integration: Providers currently have two separate logins for EHR and for PDMP, which makes accessing PDMPs cumbersome and disruptive to provider workflow. Legislation that encourages direct integration within EMRs would enable seamless reconciliation of a patient’s opioid prescription history with their current medications and healthcare needs.
4. Expanding Access to OUD Treatment and Mental Health Services
One significant barrier that patients face in seeking and sustaining treatment for OUD is a lack of financial resources and adequate healthcare coverage. This includes coverage for OUD treatment itself, and for mental health care which may be a concurrent or contributing factor to opioid addiction. Recent legislation, such as the 21st Century Cures Act, sought to address some of these challenges, but we urge Congress to further expand coverage to include coverage for Medication-Assisted Treatment (MAT) and to reconsider the 190-day lifetime limit on Medicare inpatient psychiatric hospitalizations, as part of any solution. Coverage in this case means that the health plan allows a patient to access these services, and that providers of these services are adequately reimbursed. From the hospitalist perspective, expansion of federal support for outpatient mental healthcare is critical, as lack of outpatient access to mental health providers is a contributor to OUD relapse.
5. Expand Research and Access to Non-Opioid Therapies
Congress should also consider an increase in funding and support for research into and treatment coverage of non-opioid options for pain that could decrease the reliance on opioids. This would include not only non-addictive pharmacologic options, but also multidisciplinary pain management programs involving physical therapy and psychotherapy, and non-traditional medical therapies such as massage and acupuncture. Expanded payment options for use of these options would incentivize their use as an alternative to opioid prescriptions.
[1]CDC/NCHS, National Vital Statistics System, Mortality. CDC Wonder, Atlanta, GA: US Department of Health and Human Services, CDC; 2017. https://wonder.cdc.gov.
{kind=link}
[2] Herzig SJ, Hilary J. Mosher, MD, Calcaterra SL, Jena AB, Teryl K. Nuckols, MD, Improving the Safety of Opioid Use for Acute Noncancer Pain in Hospitalized Adults: A Consensus Statement From the Society of Hospital Medicine. J. Hosp. Med 2018;4;263-271.